How to Prevent the Next Pandemic (2022) is a blueprint for the international pandemic prevention plan the world sorely needs. Learning from the mistakes of the Covid 19 pandemic, Gates lays down a series of steps governments need to take if we’re to protect ourselves and ensure another global health catastrophe of this scale never happens again.
Genres
Table of Contents
- Genres
- Introduction: Learn what it takes to prepare for a crisis.
- The countries that handled the Covid pandemic best were the ones that had plans for testing and tracing already in place.
- The world needs an international pandemic prevention team.
- A global disease surveillance system would be our first line of defense against an outbreak.
- We need to create a system that funds better tools, treatments, and vaccines.
- GERM would help organise international pandemic simulations to prepare for an outbreak.
- Tackling global health inequality is essential for protecting everyone against pandemics.
- Summary
- About the Author
- Table of Contents
- Review
Science, Politics, Medicine, Virology, Forensic Medicine, Viral Diseases,
Introduction: Learn what it takes to prepare for a crisis.
If there was one person who wasn’t surprised by the pandemic that engulfed the world in the early months of 2020, it was Bill Gates. In fact, he’s been trying to warn governments to take action against a coming pandemic for years.
Back in 2015, Gates gave a now-famous TED talk where he warned the world of how woefully unprepared we were to deal with a deadly new virus. He pushed for a solution and explained exactly what we could be doing to prepare.
![[Book Summary] How to Prevent the Next Pandemic: What We’ve Learned From COVID-19 & the Changes We Need to Make](https://lh3.googleusercontent.com/pw/AM-JKLUqK5Qkfor0ipqqMpyiciMcvgmLkG5CvoqkMfLsAkw-4bRpjXJLkPZMyT1EOVGadGVZAIp7beUSEHl07RsU4fvMx5H2BtUe04zy9FR5Ke9KcknKMN0PNSDi4luaMvzVWbMB0ihC0Vti80fYg47Kpi9ccQ=w1425-h748-no?authuser=0)
Unfortunately, hardly anyone took any notice. None of his suggestions were implemented. Gates was shocked by how little people seemed to care about this issue.
These days, of course, things have changed – Gates’s TED talk has now been viewed over 43 million times. But with 95 percent of those views coming after the Covid pandemic began, it was too little, too late.
Now that we have the benefit of hindsight, we’re all painfully aware of just how real the threat of a global pandemic actually is. But especially now, we shouldn’t become complacent. Already, the sense of urgency we felt during the height of the pandemic is starting to fade as the world turns its attention to other problems. It’s vital that we take action now and put a plan in place to deal with future pandemics before the last one becomes old news.
This summary to Bill Gates’s How to Prevent the Next Pandemic outlines exactly such a plan. Drawing on the knowledge of the world’s foremost experts in the field of epidemiology, as well as on Gates’s own experience in disease prevention through his work at the Gates Foundation, it highlights exactly where the gaps in our system are – and how we can address them to ensure another Covid-like catastrophe never happens again.
The countries that handled the Covid pandemic best were the ones that had plans for testing and tracing already in place.
Now that we’re (hopefully) at the tail end of the Covid pandemic, we have one very good reason to be optimistic that we’ll handle things better next time: experience.
Countries who had recently dealt with other outbreaks tended to perform better during this pandemic. In 2003, countries like China, Taiwan, Singapore, and Vietnam were hit hard by the SARS outbreak. When Covid struck, they all responded quickly and effectively – and were able to successfully limit new cases for over a year. Clearly, these countries did something right.
So, if we want to protect ourselves from future pandemics, a good bet is to look at – and copy – what these countries have learned through experience.
As it turns out, there are three things all these countries excelled at right from the get-go. First, they were all able to quickly ramp up testing for a large proportion of their population. Second, they all had systems in place to trace people who had potentially come into contact with the disease. And third, they isolated everyone who tested positive or had been exposed to the virus.
By contrast, the US floundered in all three of these respects simply because of its inability to fully utilize testing. Early on, this was because tests were in short supply and the country struggled to acquire the kits it needed. But even by the time the Omicron variant appeared, many people were still unable to get tested because the testing centers were so flooded.
What’s more, the US never created a centralized way to prioritize testing and share the results. This was a missed opportunity. Any software company worth its salt could have whipped up a solution in a heartbeat if it had been asked. Instead, states and cities were left to their own devices, which led to a chaotic, inconsistent rollout of testing across the country.
The bottom line is that testing is something we’ll need to prepare for in advance next time. In the early days of an outbreak, if we can test a large segment of the population, isolate those who may be infected, and trace anyone coming from abroad, we’ll be well-positioned to keep cases at a manageable level. If we don’t prepare, we might have to again resort to unpopular measures like lockdowns to prevent huge casualties.
The world has not yet properly invested in the systems and tools we need to undertake large-scale testing. It’s about time we did.
The world needs an international pandemic prevention team.
If you think about it, it’s kind of odd that we don’t have a branch of emergency services dedicated to preventing pandemics.
To put it into perspective, the US employs about 311,000 full-time firefighters across 30,000 departments throughout the country. In all, local governments spend over $50 billion a year just to have firefighting crews on call in the event of a fire. That might seem like a lot of money to prepare for an event that’s relatively rare, but it’s worth it. It’d be far more costly, in terms of both money and lives, to be unprepared if a fire did break out.
Given how much effort and money governments put into preparing for fires, it’s striking how little they put into preparing for pandemics – especially because the latest pandemic was far deadlier and more damaging to economies than any fire has ever been.
If we take fires seriously, we should be even more serious about pandemics. What we need is something equivalent to a fire department, but with the mission of stamping out diseases wherever they emerge. It would have to be a global institution because, unlike fires, pandemics are capable of spreading across any ocean and terrain to every corner of the Earth within weeks.
The only institution that currently comes close to fulfilling this role is the World Health Organization, or WHO. Unfortunately, as it stands, the WHO is chronically underfunded and has almost no full-time personnel responsible for managing pandemics. That means there’s currently no institution with the size, funding, or authority necessary to serve as an international pandemic response team.
For the sake of argument, let’s imagine what this squad of virus-fighting superheroes might look like. Let’s call them GERM, or Global Epidemic Response and Mobilization. GERM would be made up of a team of specialists whose task it is to wake up every morning worrying about one thing: Are we prepared for the next deadly outbreak?
Ideally, the GERM team would have the authorization to work with governments and the World Bank to coordinate every aspect of a pandemic response. They would be responsible for identifying potential outbreaks and raising the alarm. They would serve as a hub for global health data and use it to run computer models. And they would draw on this data to advise governments on measures to take, such as closing borders or mandating mask use.
One thing the GERM team wouldn’t be responsible for is actually treating people. GERM wouldn’t replace hospitals and national health agencies, which do important work at a national level. Their job would simply be to coordinate the patchwork of national health organizations into a single, integrated global health system. Such a system would significantly improve the world’s ability to share data and coordinate activities, which would help to avoid the chaotic “every-state-for-itself” approach we saw during COVID-19.
The GERM team would play an essential role in all aspects of pandemic prevention, which we’ll explore more in the following chapters. Let’s start with the most important one: disease surveillance.
A global disease surveillance system would be our first line of defense against an outbreak.
Disease surveillance was an obscure field for most of its existence. That changed when COVID-19 thrust it into the limelight. Of course, it would have helped to have paid more attention before we were hit by a pandemic – but better late than never.
Put simply, disease surveillance is about keeping track of diseases – detecting outbreaks and monitoring how they spread through a population. The information this provides helps with everything from shaping public policy to selecting which strain of flu to vaccinate people against each year.
It’s not as easy as it may sound. The trouble is, people are always getting sick. But not every instance of a sickness leads to an outbreak. So disease surveillants have to comb through all the cases and decide which ones seem the most likely to cause problems. It’s not like looking for a needle in a haystack – it’s like looking for a really sharp needle in a pile of blunter ones.
The trick is to keep an eye out for suspicious clusters of an illness. Clusters should immediately raise a red flag because they indicate that a pathogen is contagious and has already begun to spread. To be able to spot a cluster early, though, you need good data. Things like who got sick, what their symptoms were, and where they likely picked up the pathogen are all valuable information.
Some of that data will come from clinics and hospitals as people check themselves in. But as we know from Covid, not everyone who gets sick feels bad enough to bother getting help. That’s why it’s important in the early stages of an outbreak to be proactive with testing; that way, you can get an idea of how many mild and asymptomatic cases are out there.
Aside from testing, countries are increasingly turning to more innovative methods of gathering health data, such as scanning social media for reports of illness. For example, in Vietnam, pharmacists are instructed to file a report if sales of fever and cough medication start to increase.
Another promising new approach involves searching for pathogens directly in the environment. Many pathogens can be found in human feces, for instance, which means you can check for them in the wastewater of sewage systems. Studies show that this could be an effective way of detecting diseases even before patients start showing up at the clinic.
Collecting data is only one half of the problem. To effectively carry out disease surveillance, you need to have a system for sharing and accessing that data over large regions. In Africa, a system like this already exists. It’s called the Disease Surveillance and Response System, and it enables countries across the continent to aggregate their data on certain diseases such as malaria and AIDS. This is invaluable for people who do disease surveillance because it means they can compare regions and track the spread of diseases.
We need this kind of system – but for the whole planet. This is where our fictional GERM team comes in. They would be the hub for global health data. And they’d share access to that data with everyone. It would mean an outbreak could be detected on one continent and immediately set off the alarm on all the others.
With this kind of infrastructure in place, we’d be much more likely to detect a new disease before it spread too far. In turn, we’d have a much higher chance of containing the outbreak – and more time to prepare before it got out of control.
We need to create a system that funds better tools, treatments, and vaccines.
Disease surveillance is the first defense in any pandemic prevention plan. If we have any hope of stopping a disease, we obviously first need to know that it exists. The next step would be to roll out treatments and vaccines to combat the disease as quickly as possible.
Now, if there’s one thing we got right during Covid – which surprised even the experts – it was this aspect. The fact that scientists were able to design multiple vaccines in the space of a year was unprecedented in the history of medicine. But what was even more miraculous was the sheer speed and scope with which we managed to get them into people’s arms all over the world. Vaccines really were the great success story of the whole Covid pandemic.
Even so, we can do better – and we’ll need to if we want to avoid large-scale lockdowns again. Ideally, vaccines would go from the lab to the public within six months of identifying a dangerous pathogen. This is achievable if we can find innovative ways to speed up the development, manufacturing, and delivery of vaccines without skimping on safety.
But we can’t expect innovation to just happen by itself. Innovation usually takes years of painstaking research, and that requires funding. The Covid vaccines, for example, were the result of decades of research into mRNA technology and other cutting-edge science.
What we need is a system for nurturing innovation in health care. Again, our friends at GERM could be the answer. The GERM team could oversee and coordinate research all over the world. They could also help funnel government funding into the most promising new ideas.
Just to give you a sense of the range of exciting new technologies already in the pipeline, let’s look at some of the things researchers are currently working on.
One area that’s rife with new ideas is vaccine delivery. Researchers are looking into the possibility of creating vaccines that don’t require needles. Instead, they might be administered using nasal sprays or even by placing a micro-needle patch on your arm – sort of like a nicotine patch. Just imagine: in the future, you could be buying vaccines over the counter and applying them yourself!
Other promising areas of research include vaccines that don’t need to be kept cold, ones that only require a single dose, and others that would protect not just against one strain of a virus, but against entire virus families. If we can get these innovations off the ground, it would revolutionize our capacity to vaccinate people, especially in poorer countries.
In the end, this chapter boils down to two main points. First, the world is lucky that we were able to produce vaccines against Covid so quickly – and that’s definitely something to celebrate. But second, we’ve only scratched the surface of what we can achieve with vaccines. Since we can’t assume we’ll be so lucky next time, we should pursue an ambitious research agenda right now to improve vaccine technology as quickly as possible.
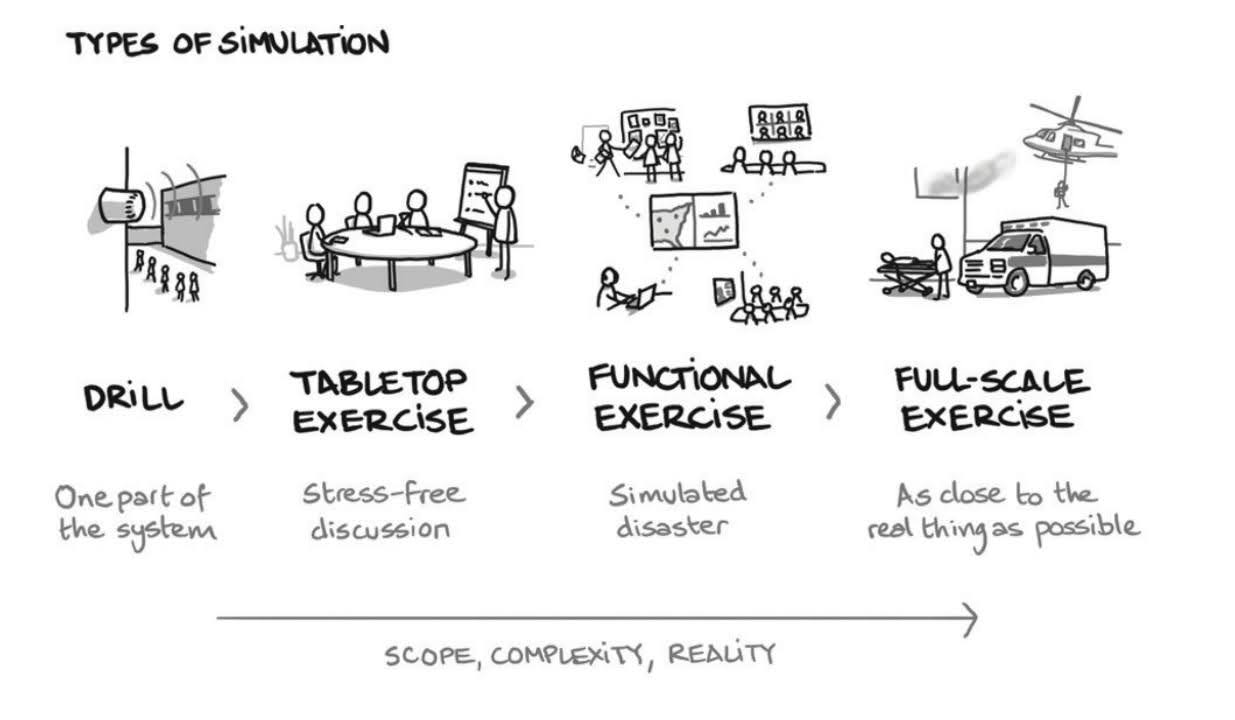
GERM would help organise international pandemic simulations to prepare for an outbreak.
Part of the reason we were caught so off guard by Covid was that we’d grown complacent. We hadn’t experienced a truly devastating pandemic, at least not in the West, since the 1918 influenza – and that was a hundred years ago. We can’t allow time to make us so complacent again.
Fortunately, there’s an easy way to solve this problem. We can run periodic practice exercises to test our global response systems and keep them alert.
Exercises like this are already commonplace for other kinds of crises. Militaries, for example, run war games to prepare for a possible invasion. Airports run drills in the event of a plane crash or a terrorist attack. And local governments run city and state-wide exercises to prepare for natural disasters such as earthquakes and tsunamis.
One of the most famous of these is called Cascadia Rising. This is a periodic full-scale drill designed to test the readiness of the Pacific Northwest for the next mega-earthquake, which is due anytime now. When the last drill took place back in 2016, thousands of people were involved – including dozens of government agencies, private businesses, and the military.
But when it comes to pandemics, real-world practice exercises like these just don’t seem to happen. It’s true, there are a few countries that are ahead of the curve. Indonesia deserves credit for running what was probably the world’s first full-scale outbreak exercise back in 2008. Still, events like this are absent in most regions of the world.
This is another area in which our GERM team could help out. GERM could coordinate with governments, national health institutions, and military leaders to help them undertake these exercises. They could give advice, review their performance, and even provide resources for countries that need them.
Here’s what a full-scale outbreak exercise might look like. First, you’d choose the city or region to test. Then you’d sprinkle in a few fake reports of a serious illness by, say, asking volunteers to report symptoms at their nearest clinic. Once the alarm’s been raised, you would then monitor the region’s progress as it sets up systems for testing new cases, analyzing the pathogen, and reporting this data.
After the exercise is complete, GERM would review the findings, identify weak points in the system, and distill these into a list of recommendations. These might include things like how to strengthen supply chains and distribute medicines, or offering more efficient methods to conduct testing and data collection. If necessary, GERM could also put political pressure on leaders to translate these recommendations into action.
Hopefully we’ve learned from our experience with Covid, and will start treating pandemics with the same gravity we treat earthquakes and other disasters. We can’t control when a disaster will strike. But we can practice how we’ll respond to one when it happens.
Tackling global health inequality is essential for protecting everyone against pandemics.
There’s a big elephant in the room that needs to be addressed before we wrap up – and that elephant is inequality. Another lesson many of us learned the hard way during Covid is that the pandemic didn’t affect everybody equally.
Within the US, Black, Latino, and Native American people were twice as likely to die during the pandemic than white people. On an international level, the situation was just as dire. In 2020, nearly 100 million people around the world were forced into extreme poverty – the first time global poverty has gone up in decades.
And those who were most affected by the pandemic were also those who received the least help. People in low-income countries were far less likely to be tested or treated for Covid. When it comes to vaccines, the disparity is even more dramatic. Of the 10 billion vaccine doses that have so far been administered, only 1 percent of those have gone to people in low-income countries.
Many people in the West were rightfully shocked and outraged by this disparity. How is it that the world can produce enough doses to vaccinate everybody – and yet not distribute them equally? But the truth is, this inequality is nothing new. The Covid pandemic was simply the latest event to highlight a deep-seated health disparity between the developed and developing worlds.
Consider that many people in Sub-Saharan Africa die from diseases that rarely kill people in North America. Over the past decade alone, 4 million children in Sub-Saharan Africa have died from malaria, while in the US only 100 people died from the disease in the same period. And millions more in Africa die every year from other preventable diseases or during childbirth.
A child born in Nigeria is 28 times less likely to see her fifth birthday than a child born in the US. Where you’re born in the world determines to a great extent your chances of growing up to adulthood. This will still be true once the Covid pandemic is over and done with.
We’re not trying to depress you – but this is a problem that deserves more attention! Part of the difficulty is that basic health-care infrastructure in many low-income countries is often very limited. That means that vital medical resources, such as drugs, vaccines, and treatments, simply can’t reach the people who need them.
The governments of wealthier countries can help to solve this problem by investing more in the health infrastructure of poorer countries. Rich countries should do this not only because it’s the morally right thing to do, but because it’s in their interest for foreign countries to have a robust health-care system.
As Covid made clear, pathogens don’t care about human borders. What happens in one region of the world can have consequences for every other. If a pathogen in one country can’t be controlled due to a lack of tools to detect or contain it, it will likely spread to other countries too.
Conversely, when we strengthen local health systems, we increase our chances of catching new pathogens early – before they turn into pandemics. It also helps us vaccinate people more efficiently when the time comes.
Ultimately, closing the global health gap is a long-term project. We’re not going to solve inequality overnight. But that’s exactly why it’s essential to start now. The earlier we try to tackle this problem, the better prepared we’ll be the next time everything goes awry.
Summary
This summary has very much focused on the big picture – and that’s because there’s a huge role that big institutions, like governments and our fictional GERM team, will need to play in order to control the spread of disease on a global scale. On the individual level, it may seem like there’s not much you can do to influence the course of a pandemic.
But that’s not true. Pandemics are caused by the cumulative actions of many individuals, so there are plenty of ways you can help keep your community safer.
For one, you can do your part in following any health and safety guidelines that may be put into place during an emergency – like wearing a mask, social distancing, and getting vaccinated as soon as you’re able to. You can also help by electing leaders who value science and will take advice from experts when the time comes.
But, most of all, you can help to keep health and disease prevention on the agenda by not letting the world forget just how devastating Covid was. Sure, we all can’t wait to put Covid behind us, but there’s one thing we simply can’t afford to do: return to being complacent about pandemics.
That doesn’t mean we have to live in perpetual fear of another deadly outbreak. It just means we have to understand that another pandemic is possible – and be willing to do what we know it takes to prevent it.
About the Author
BILL GATES is a technologist, business leader, and philanthropist. In 1975, he cofounded Microsoft with his childhood friend Paul Allen. Today, he is cochair of the Bill & Melinda Gates Foundation, where he has spent more than twenty years working on global health and development issues, including pandemic prevention, disease eradication, and problems concerning water, sanitation, and hygiene. He has three children.
Table of Contents
Introduction
1 Learn from COVID
2 Create a pandemic prevention team
3 Get better at detecting outbreaks early
4 Help people protect themselves right away
5 Find new treatments fast
6 Get ready to make vaccines
7 Practice, practice, practice
8 Close the health gap between rich and poor countries
9 Make—and fund—a plan for preventing pandemics
Afterword: How COVID changed the course of our digital future
Glossary
Acknowledgments
Notes
Index
Review
The book is divided into three parts: The Lessons of COVID-19, The Road to Zero, and The Future of Health. In the first part, Gates analyzes the causes and consequences of the COVID-19 pandemic, highlighting the failures and successes of the global response. He identifies six key lessons that we should learn from this experience:
- We need to rapidly scale up testing and tracing to detect and contain outbreaks.
- We need to invest in vaccine research and development, as well as manufacturing and distribution, to ensure equitable access for all.
- We need to strengthen our health systems and workforce, especially in low- and middle-income countries, to cope with surges in demand and prevent health inequities.
- We need to improve our international cooperation and coordination, as well as our preparedness and resilience, to prevent and respond to future pandemics.
- We need to address the root causes of zoonotic diseases, such as deforestation, wildlife trade, and factory farming, to reduce the risk of spillover events.
- We need to tackle the climate crisis, which exacerbates the spread and severity of infectious diseases, as well as other health threats.
In the second part, Gates lays out his vision for achieving zero COVID-19 cases and deaths worldwide, as well as zero respiratory diseases in general. He argues that this is not only possible, but also necessary, for the sake of human health and well-being. He proposes a four-step plan to reach this goal:
- We need to end the acute phase of the pandemic by vaccinating at least 70% of the global population and implementing public health measures such as masking, social distancing, and ventilation.
- We need to eliminate community transmission of COVID-19 by using genomic sequencing, digital tools, and targeted interventions to track and stop every case.
- We need to eradicate COVID-19 by developing new vaccines that can protect against all variants and strains of the virus, as well as ensuring universal coverage and booster doses.
- We need to prevent respiratory diseases by developing universal vaccines that can protect against multiple pathogens, such as influenza, RSV, and pneumococcus, as well as improving hygiene, nutrition, and environmental quality.
In the third part, Gates explores the future of health in a post-pandemic world. He envisions a world where everyone has access to quality health care and prevention services, where innovation and technology are harnessed for good, where health equity and justice are prioritized, and where health is seen as a global public good. He also discusses some of the emerging challenges and opportunities that we will face in the coming years, such as aging populations, antimicrobial resistance, bioterrorism, synthetic biology, artificial intelligence, and digital health.
The book is a timely and insightful contribution to the ongoing debate on how to prevent the next pandemic. Gates draws on his extensive experience and expertise in global health, philanthropy, and innovation to offer a comprehensive and compelling analysis of the current situation and the future prospects. He combines scientific data, personal anecdotes, historical examples, and practical recommendations to make his case for a bold and ambitious agenda for change. He also acknowledges the limitations and uncertainties of his arguments, as well as the potential trade-offs and ethical dilemmas involved.
The book is written in a clear and accessible style that engages the reader throughout. Gates uses simple language, analogies, metaphors, charts, graphs, maps, photos, and illustrations to explain complex concepts and convey his messages. He also injects humor, optimism, and empathy into his writing, making it more relatable and inspiring. He addresses some of the common questions and concerns that people may have about his proposals, such as their feasibility, cost-effectiveness, safety, equity, acceptability, and sustainability. He also invites feedback from his readers through his website and social media platforms.
The book is not without its flaws or criticisms. Some may find it too optimistic or unrealistic in its assumptions or projections. Some may disagree with its priorities or perspectives on certain issues or solutions. Some may question its sources or evidence base or its balance or objectivity. Some may challenge its authority or credibility or its motives or interests. Some may point out its gaps or omissions or its contradictions or inconsistencies. Some may argue that it does not go far enough or fast enough or deep enough in addressing the root causes or systemic factors that contribute to pandemics.
Overall, however, the book is a valuable and influential resource for anyone who is interested in learning more about pandemics and how to prevent them. It is also a powerful call to action for everyone who cares about health and humanity. It challenges us to think big and act boldly in pursuit of a healthier and safer world for ourselves and future generations. It reminds us that we are all connected and interdependent in this globalized world. And it urges us not to waste this opportunity to learn from COVID-19 and make the changes we need to make.